Authors: Marcos Ballester, Geoffroy Canlorbe, Annie Cortez, Julie Gonin, Enora Laas, Olivier Graesslin, and Emile Darai.
 |
| Image found at MyHealth.Alberta.ca |
Endometrial cancer (EC) is the most common cancer of the female reproductive tract and is also the fourth most common cancer affecting the developing countries. It is characterized by malignancies that arise solely from the endometrial lining of the uterus, unlike other uterine cancers, such as ovarian or cervical cancer, where the cancer arises from other tissues of the uterus.
 |
| "Figure 1" found at this website |
There are two types of endometrial cancer: the more common carcinomas, that originate from a single layer of the epithelium; and the lesser known sarcomas, that arise from non-glandular connective tissue in the endometrium (Hoffman, B.L.,
2012). Early stage endometrial cancer
has three risk groups: low, intermediate and high, however as of yet, there is
no clear criterion to define or distinguish them. Many procedures have been
used to determine survival and prognosis, the most common being preoperative
procedures that stage the cancer and determine the course of action to get rid of it.
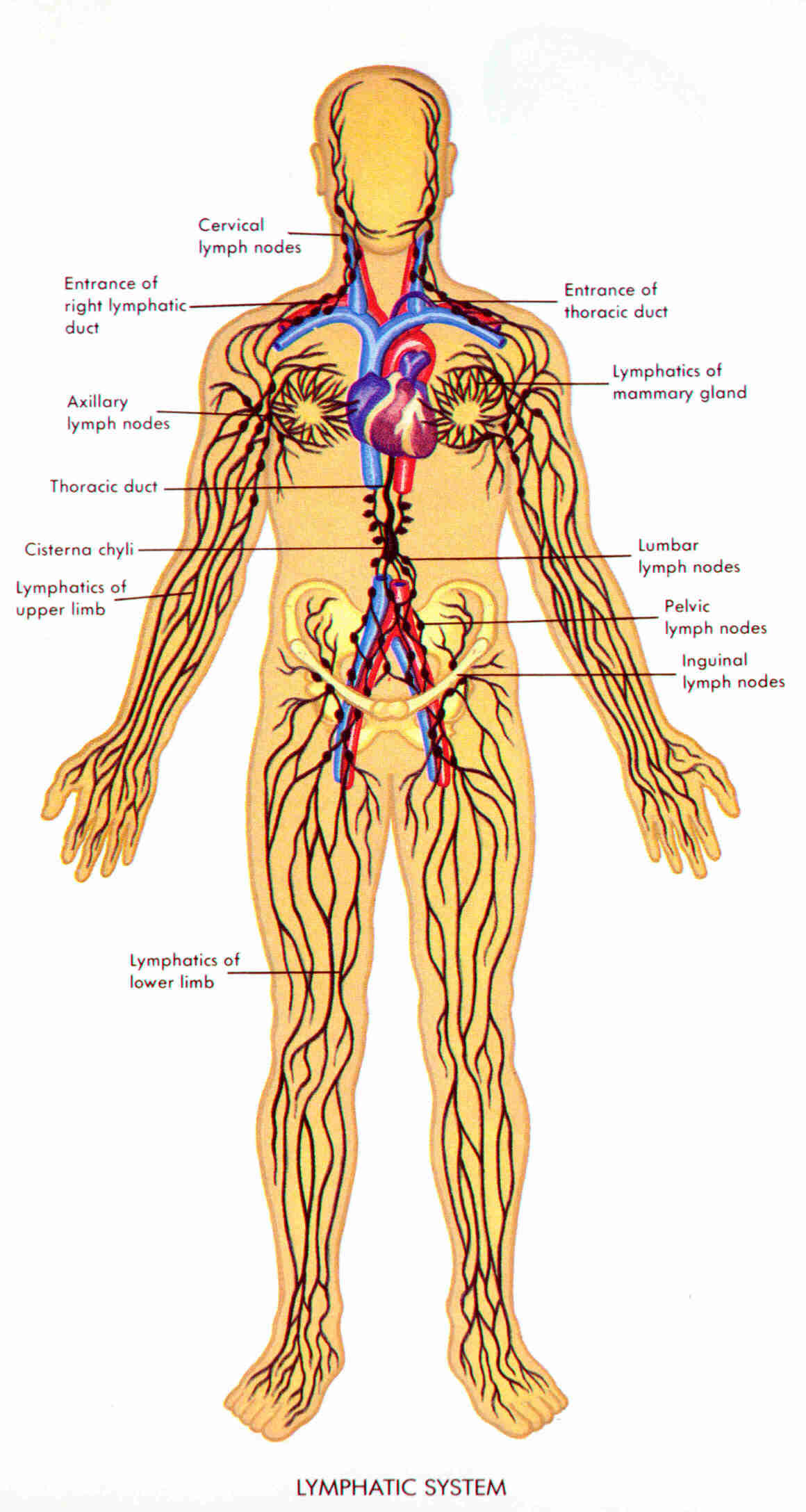
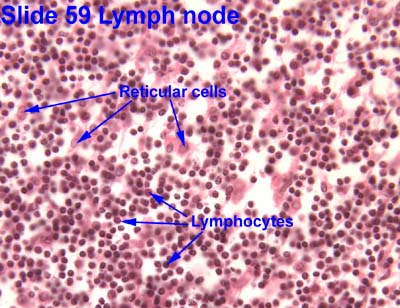
Checking lymph node
status is one method that estimates the survival of the patients
and involves analyzing the lymph nodes for histological clues such as the grade
of the tumour (see criteria below) or the depth of the myometrial invasion. Myometrial invasion refers to the degree at which the tumor has invaded the smooth muscular lining of the uterus.
Many different procedures have been utilized to check lymph node status, however very few are currently considered entirely "safe". Pelvic lymphadenectomies involve dissecting the lymph nodes of the pelvic region to see whether the cancer has remained contained within the pelvic region or spread to other organs in the body, a process known as metastasis (Wagman, L.D., 2008). This procedure is no longer recommended for low-intermediate risk women due to the high risk of post-operative morbidity and low-effectiveness in the early stages of the cancer.
A sentinel node biopsy is another procedure which involves injecting a radioactive substance and dye molecules into the area in close proximity to the tumor. The lymph nodes is observed for colour change or dye uptake and are also assessed for radioactivity to see whether any node has absorbed any of the previously injected radioactive substance. Once the affected lymph nodes are detected, they become known as "sentinel lymph nodes" and are dissected and sent for analysis to detect the presence of cancer (Wagman, L.D., 2008). It is hypothesized that sentinel lymph nodes are the first lymph node group to drain metastasizing cancer cells and will thus be the first area where metastases will be discovered. In a previous study by Ballester et. al., it was reported that sentinel node biopsies can detect metastasized cancer cells in 10% of low-risk patients and 15% in high-risk patients. This procedure has many advantages, including early detection and the ability to replace full lymph node dissections, however, it is not scientifically proven that an early stage sentinel node biopsy is any more effective at increasing survival rate than waiting until a later stage and feeling the lymph nodes for enlargements (Thomas, J., 2008).
Once the cancer has been staged, physicians can decide how to proceed. Surgical treatment is a common strategy if necessary, however surgical intervention is quite intense and invasive. Generally, women must undergo a total hysterectomy (removal of the uterus) and a bilateral salpingo-oophorectomy (the surgical removal of both ovaries and both Fallopian tubes) in order to be confident that all the cancer has been removed (that is, if it hasn't already metastasized). Both of these procedures are major surgeries with associated complications and long healing times. Usually, these approaches are only recommended when all other options have been exhausted, especially because of the inability to reverse the procedure, leaving the woman unable to bear children, and the risk for many other health problems following the surgery.
Many different procedures have been utilized to check lymph node status, however very few are currently considered entirely "safe". Pelvic lymphadenectomies involve dissecting the lymph nodes of the pelvic region to see whether the cancer has remained contained within the pelvic region or spread to other organs in the body, a process known as metastasis (Wagman, L.D., 2008). This procedure is no longer recommended for low-intermediate risk women due to the high risk of post-operative morbidity and low-effectiveness in the early stages of the cancer.
A sentinel node biopsy is another procedure which involves injecting a radioactive substance and dye molecules into the area in close proximity to the tumor. The lymph nodes is observed for colour change or dye uptake and are also assessed for radioactivity to see whether any node has absorbed any of the previously injected radioactive substance. Once the affected lymph nodes are detected, they become known as "sentinel lymph nodes" and are dissected and sent for analysis to detect the presence of cancer (Wagman, L.D., 2008). It is hypothesized that sentinel lymph nodes are the first lymph node group to drain metastasizing cancer cells and will thus be the first area where metastases will be discovered. In a previous study by Ballester et. al., it was reported that sentinel node biopsies can detect metastasized cancer cells in 10% of low-risk patients and 15% in high-risk patients. This procedure has many advantages, including early detection and the ability to replace full lymph node dissections, however, it is not scientifically proven that an early stage sentinel node biopsy is any more effective at increasing survival rate than waiting until a later stage and feeling the lymph nodes for enlargements (Thomas, J., 2008).
Once the cancer has been staged, physicians can decide how to proceed. Surgical treatment is a common strategy if necessary, however surgical intervention is quite intense and invasive. Generally, women must undergo a total hysterectomy (removal of the uterus) and a bilateral salpingo-oophorectomy (the surgical removal of both ovaries and both Fallopian tubes) in order to be confident that all the cancer has been removed (that is, if it hasn't already metastasized). Both of these procedures are major surgeries with associated complications and long healing times. Usually, these approaches are only recommended when all other options have been exhausted, especially because of the inability to reverse the procedure, leaving the woman unable to bear children, and the risk for many other health problems following the surgery.
Although the two previously
outlined procedures for checking lymph node status are used to stage cancer
severity, additional tools are needed to safely assess prognosis and surgical
strategies in low-intermediate risk endometrial cancer patients with lymph node
metastases. This study evaluates whether or not there is a safer approach to profile low-intermediate risk endometrial cancer patients and predict their lymph node status, primarily using histological or
immunohistochemical techniques.
Methods:
The subjects used for this study were 68 women with primary endometrial cancer from the Department of Gynecology of Tenon Hospital in Paris, France who had undergone surgical treatment between June 2006 and December 2012. Medical records revealing age, surgical history, histological type and tumour-grade, depth of myometrial invasion and incidence of lymphovascular space invasion were reviewed in order to determine eligibility for the study. Surgical history was a controlled variable, since each of the women had experienced a preoperative biopsy and MRI of the endometrium to assess cancer stage, histological type, tumor grade, etc., and were staged based on the 2009 International Federation of Gynecological Obstetrics (FIGO) report (see outlined FIGO below). The subjects were also required to have undergone surgical intervention in the form of a pelvic lymphadenectomy, total hysterectomy and a bilateral salpingo-oophorectomy to be considered for this study.
The FIGO rates cancers as
follows:
Type I: endometrial tumors of one of the following grades:
- Grade 1: less than or equal to 5% non-squamous nonmorular-solid growth (cancer cell has not developed past the blastomere stage to become a solid mass)
- Grade 2: 6-50% nonsquamous non-morular-solid growth
- Grade 3: >50% nonsquamous non-morular-solid growth
Type 2 are classified as clear carcinomas, serous carcinomas and
carcinosarcomas (which will be excluded from this study)
 |
| Figure obtained from Jobson Publication's U.S. Pharmacist "Endometrial Cancer: Updates in Pharmacotherapy" |
Once the type and grade of the cancer has been identified, the risk scale can be defined:
- Low risk is defined as Type 1 endometrial cancer with FIGO stage IA
grade 1 or 2.
- Intermediate risk is define as Type 1 endometrial cancer with FIGO
stage IA grade 3 or IB stage 1 or 2.
 |
| Figure obtained from the National Cancer Institute's "Endometrial Cancer Treatment" page |
This study also considered the incidence of Lymphovascular space invasion (LVSI),
which is the incidence of cancerous tissue within the lymph node spaces lined
with endothelial cells. Women were classified as either LVSI-positive
(cancerous tissue present in the lymph node spaces) or LVSI-negative (no
cancerous tissue in the lymph node spaces).
To test immunohistochemistry, biopsied
tissues were fixed with formalin, processed in paraffin blocks and stained with
rabbit monoclonal antibodies directed against estrogen (ER) and progesterone (PR) receptors. A universal biotinylated immunoglobulin was used as a secondary
antibody and positive controls of ER and PR were sectioned from breast tissue. This
method works by immunological mechanisms. In brief, when a particular tissue
contains an antigen that is specific for the monoclonal antibody used in the
immunoassay (usually something like an ELISA), the two will bind together and
form a precipitate or a colour change, indicating a positive match. This
positive match indicates that the tissue being tested contains the antigen
specific for the monoclonal antibody. In this case, if a positive match occurs,
the tissue will have the specific estrogen or progesterone receptors that are specific for the estrogen/progesterone receptor monoclonal antibodies
circulating in the stain.
Results:
Ballester et. al. found the following final histological grade results when there were exactly 34 cases of low-risk patients and 34 cases of intermediate-risk patients: 32 cases (47% of women) had Grade 1 EC, 29 cases (43% of women) had Grade 2 EC and 7 cases (10% of women) had Grade 3 EC. For myometrial invasion depth, over 53% (36 cases) had less than 50% invasion depth and 47% (32 cases) has more than 50% invasion depth. Of the 68 participants, 25 women were LVSI-positive and 19 had metastatic lymph nodes (3 in low-risk group and 16 in intermediate-risk groups). Of these, there were 14 cases of macrometastases, 3 cases of micrometstases and 2 cases of isolated tumor cells found, however these types of metastases do not have very many studies surrounding the survival or prognosis, so they will not be considered.
Table 1: Comparison of ESMO risk group, LVSI, and estrogen/progesterone receptors
immunostaining between patients with and without lymph node metastases.

The immunohistochemical
results showed that there was lower immunostaining of ER and PR in women with
lymph node metastases (see Figure 1).
 |
| Fig. 1. Comparison of semi-quantitative estrogen and progesteron receptors immunostaining between women with and without lymph node metastases. |
Using previously determine optimal cut-offs of strongest
correlation (Figure 2) of 30% for ER and 15% for PR, the researchers compared the
ER and PR expression in women with and without lymph node metastases. They
found that more than 30% immunostaining (above optimal cut-off) was common in
women without metastases (69%) rather than those with (37%). Similarly, more
than 15% immunostaining (above optimal cut-off) was common in women without
metastases (73%) compared to those with metastases (43%). It was also found
that intermediate-risk patients and those with LVSI were more likely to have
lymph node metastases, and therefore had less immunostaining of PR and ER
receptors.
 |
| Fig. 2. Optimal cut-offs denoting a correlation between estrogen and progesteron receptors semi-quantitative immunostaining and final lymph node status. |
A recursive partitioning model
was constructed in order to create a “decision tree” of sorts that helps to
classify the women of the study based on particular variables, based on the
standard of the European Society of Medical Oncology (ESMO) (Figure 3). This RP
model predicted the absence of metastases 100% of the time when ER was
overexpressed in low-risk EC patients. The model also predicted present lymph
node metastases 88% of the time in intermediate-risk groups when there was LVSI
and low PR expression. The rest of the combinations can be viewed in Figure 3. When the model was tested for specificity and
sensitivity, the misclassification rate for shown to be 20%, indicating that
the model is fairly good at predicting the risk of endometrial cancer based on
immunohistochemical methods.
 |
| Fig. 3. Recursive partitioning model illustrating histological and immunostaining profiles to predict final lymph node status. |
Conclusions:
Ballester and his team found that women with lymph node metastases exhibit different histological/immunohistochemical profiles than those without and that final lymph node status can be accurately predicted using a combination of these techniques. The construction of the predictive model helps physicians with the important question of whether or not to opt for a lymphadenectomy and that a combination of estrogen and progesterone expression can provide an accurate predictor of lymph node status in women with low risk ER overexpression. This is because women who have lymph node metastases do not react to the immunostaining procedure as strongly as those without because these women have less estrogen and progesterone receptors for the monoclonal antibodies to bind with. In women with intermediate-risk, it is important to look at the incidence of LVSI to distinguish the women with/without lymph node metastases, this is because women with lymph node metastases are also likely to have cancer cells invading their lymphovascular spaces.
The
authors admit that lymphadenectomies and sentinel lymph node biopsies are
procedures that are accurately used to stage cancer, and when
considering low-intermediate risk groups, there is a chance that metastases
would have been overlooked had lymph node staging not occurred. However, these
procedures are still considered very risky for low-intermediate risk groups
and the newly found combination of histological/immunohistochemical techniques described by this paper can be used instead of the
dangerous procedures to predict the presence of lymph node metastases with
relatively high accuracy. Further tests into the effectiveness of using the
immunohistochemical ER and PR profiles in the predictive model in combination
with histological techniques (grade, depth of myometrial invasion and presence
of LVSI), may enable physicians to one day estimate the final lymph
node status in low-intermediate risk women with endometrial cancer using this
safer method.
Personal Critique:
I thought this paper was pretty interesting and learned a lot about endometrial cancer. For one thing, I didn’t realize endometrial cancer was so prevalent and that the procedures used to get rid of it were so risky. I feel like this paper does a great job in attempting to create new strategies for staging endometrial cancer that could replace the invasive procedures such as lymphadenectomies and hysterectomies, however, I feel like this is where my good review of the paper ends.
One thing I found particularly challenging about this paper is that a lot of the terms were not defined and I had to go to outside sources to discover what they meant, for example, I had to look up terms such as lymphadenectomy and salpingo-oophorectomy and I did a bit of research into the sentinel node biopsy and how to perform a lot of the outlined procedures. I assume that since this paper was published in a Gynecological Journal, the authors expect their readers to know what these terms mean. This is fair, however, as a reader with no real background on the topic of gynecology, I found that this was one of the paper’s shortcomings. Perhaps a simple glossary of terms would suffice for readers like me who are not comfortable with the gynecological jargon. Likewise, I did not think that the explanation of the immunohistochemistry section was very informative or detailed. I was only able to understand this section and sort of explain it in this blog due to the immunology course I took last semester. Another thing I did not like about this paper is that I found the figures uninformative, particularly because they were nowhere near where they were referenced within the text and the titles were over-simplified and lack-luster.
There were also quite a few
limitations to the experiment itself, not including those listed in the Discussion
section of this paper. For
one thing, this paper only used subjects from one particular hospital to test
their new staging model. If they truly wanted to test the accuracy of this
model, they should have applied it to different hospitals to see if its accuracy
applied elsewhere because they are not getting a representative sample! Similarly,
calling a 20% misclassification rate a “fairly high accuracy in classification”
was generous. If you consider that 20% means that 20 out of 100 people will be
misclassified, it does not seem that impressive. My fear is that people will undergo this procedure expecting high accuracy and 20% of women will end up being misclassified, probably having to undergo the
other risky procedures the researchers were trying to avoid in the first place to combat an even further gone cancer.
One good thing you can say about
this study though, is that although there is an issue with sensitivity/specificity,
the results did seem to follow the claims that a combination of both
histological (grade, depth of myometrial invasion and testing for LVSI) and
immunohistochemical techniques could help stage the endometrial cancer risk. From
the results they outlined, it did seem possible to stage cancer risk based on
the ER and PR receptors, when used in combination with the other histological
techniques. I hope for the sake of all women (not just those currently affected
by endometrial cancer) that this study provides a stepping stone into a broader
study on new procedures that can replace the current ones.

References:
1. Ballester, M., Canlorbe, G., Cortez, A., Gonin, J., Laas, E., Bendifalah, S., Grasselin, O., Darai, E. 2013. Histological and immunohistochemical profiles predict lymph node status in women with low-intermediate risk endometrial cancer. Gynecologic Oncology. 130: 457-462.
2. Ballester, M., Dubernard, G., Lecuru, F., Heitz, D., Mathevet, P., Marret, H. 2011. Detection rate and diagnostic accuracy of sentinel-node biopsy in early stage endometrial cancer: a prospective ulticentre study (SENTI_ENDO). Lancet Oncology. 12: 469-476.
3. Hoffman, B.L. 2012. Williams Gynecology: Chapter 33, Endometrial Cancer. 2nd edition. New York: McGraw-Hill Medical. 2012
4. Thomas, J. 2008. Prognostic false-positivity of the sentinel node melanoma. National Clinic for Practical Oncology. 5(1): 18-23.
5. Wagman, L.D. 2008. Principles of Surgical Oncology from Wagman et.al.'s Cancer Management: A Multidisciplinary Approach. 11th edition.













{kind=link}
{kind=link}
{kind=link}
{kind=link}